
Rushdy Ahmad (left) and the research team worked with staff at the Public Health Laboratory-Ivo de Carneri on the Tanzanian island of Pemba to obtain blood samples from patients with suspected tuberculosis for the study.
Credit: Rushdy Ahmad
Health
A timely triage test for TB
New blood monitoring could be used to help people infected with tuberculosis
More than 10 million people around the world have active tuberculosis (ATB), and every year more than a million die from it. The majority of patients live in low-resource countries where diagnosing ATB is especially challenging, as newer tests require expensive lab equipment that is frequently not available, and the historic standard of culturing a sputum sample is slow and often not sensitive enough to correctly identify ATB, meaning that many patients whose disease needs treatment are not identified until it is too late.
To help ill patients at highest risk for having ATB get the care they need, the World Health Organization (WHO) has called for the creation of a triage test that is blood-based rather than sputum-based (minimizing the infrastructure required to deploy it) and can identify patients who are at high risk for ATB and should be given a diagnostic test.
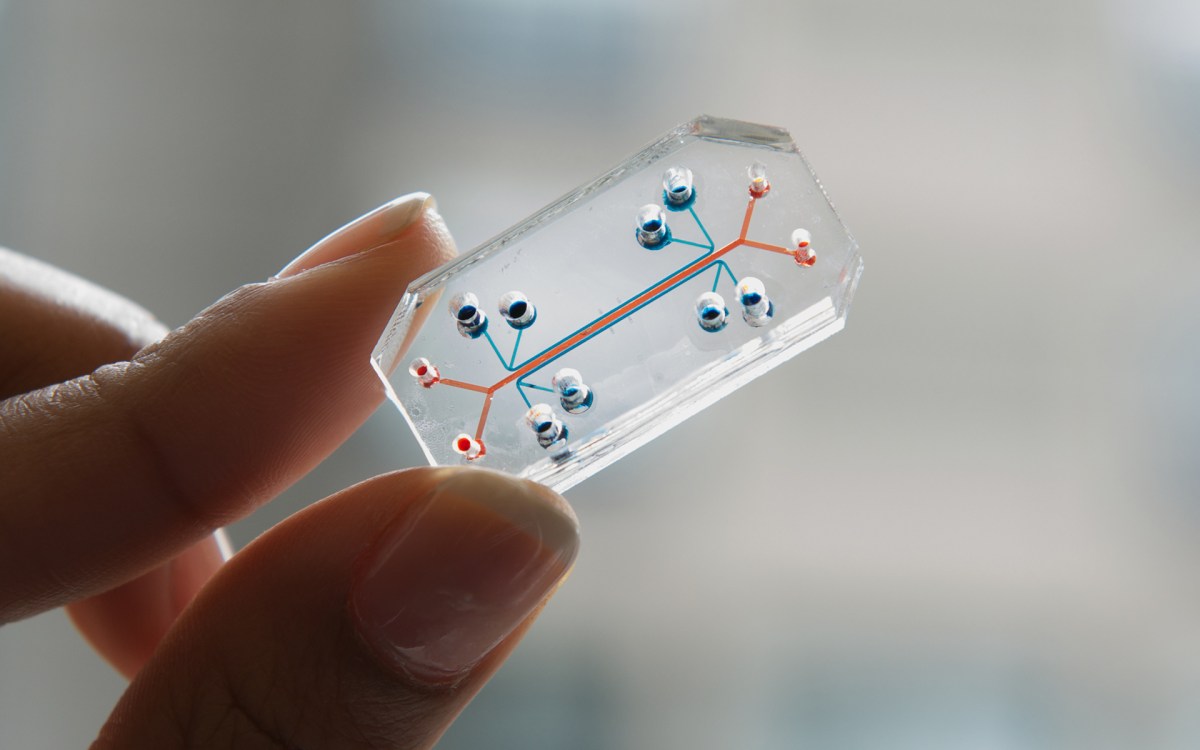
Now, a team of researchers from the Wyss Institute for Biologically Inspired Engineering, the Broad Institute of MIT and Harvard, Brigham and Women’s Hospital, and several other collaborating institutions has answered that call with a fast, ultrasensitive, multiplexed blood-based TB triage test that analyzes a “signature” of the combined levels of four proteins and an anti-TB antibody in blood samples to identify patients who are likely to have ATB and require advanced diagnostics and treatment. It can be configured into a point-of-care test that costs only $2 and gives results in about 30 minutes, lowering the barrier to care in low-resource settings and potentially saving millions of lives. The research is reported in Science Translational Medicine.
“Our test demonstrated 86 percent sensitivity and 69 percent specificity, which are very close to the WHO’s minimum requirements of 90 percent sensitivity and 70 percent specificity for an effective TB triage test,” said first author Rushdy Ahmad, a former research scientist at the Broad Institute who is now president of True North Bio. “It also effectively identified the ATB signature in patient samples from three different continents, meaning it can detect many strains of the pathogen, and in both HIV-positive and HIV-negative samples, making it widely applicable to most ATB patients.”
Protein power
The research team set out to create their blood-based test by identifying a signature set of biomarkers in patients’ blood that consistently indicated a high likelihood of ATB, then developing an easily deployable assay that could detect that signature.
They first measured the levels of 47 different blood proteins in about 400 samples taken from people in Tanzania and the Philippines who had been diagnosed with either ATB or a condition other than TB (OTB) using a traditional microbiologic assessment. Then they analyzed the protein level data using a machine-learning algorithm that honed in on four proteins that were consistently elevated in patients with ATB. Based on this signature, the algorithm correctly predicted the presence of ATB in 86 percent of all the positive samples (sensitivity), and its absence in 65 percent of the negative samples (specificity). It also correctly identified ATB in 100 percent of the samples that were HIV-positive, and the absence of ATB in 84 percent of samples from people who had been cured of ATB.
To improve their test’s ability to detect very low concentrations of the four proteins, they developed an ultrasensitive immunoassay on the Simoa platform that enabled effective measurement of protein levels using as little as a drop of blood from a fingerprick. This assay improved the algorithm’s sensitivity to 87 percent and the specificity to 66 percent. In addition, the test did not predict ATB in 19 samples that had latent TB, demonstrating that it is effective at triaging patients who need immediate medical attention from those whose disease does not require expensive intervention.
“Elevated levels of all four of the blood proteins we analyzed have been identified in a range of different diseases, but only when combined into a predictive algorithm do they have the power to distinguish ATB from other conditions,” said co-corresponding author David Walt, a core faculty member of the Wyss Institute who is also the Hansjörg Wyss Professor of Biologically Inspired Engineering at Harvard Medical School (HMS) and a senior investigator in the Department of Pathology at the Brigham.

Faster, better, cheaper
For the second phase of the study, the research team validated their algorithm by testing its ability to identify ATB in a different set of 317 samples taken from patients in Vietnam, South Africa, and Peru. They also tested a fifth biomarker in this cohort of samples to improve the algorithm’s performance: the presence of antibodies against the TB antigen Ag85B. With this added parameter, the test was able to achieve 86 percent sensitivity and 69 percent specificity. It also retained its performance in HIV-positive and -negative samples, as well as samples with latent TB.
“Not only is this method one of the fastest and most accurate ATB triage tests available, it is also much more amenable to deployment in low-resource communities than other existing approaches, it works on patients with different strains of TB, and its results are not complicated by HIV infection status,” said co-corresponding author Michael Gillette, a research scientist and senior group leader of the Proteomics and Biomarker Discovery program at the Broad Institute who is also an assistant professor of medicine at HMS. “These qualities give it the potential to be a lifesaver by identifying patients who need a diagnostic TB test right away, which would reduce both deaths from undiagnosed ATB and overuse of antibiotics and expensive diagnostics on non-ATB patients.”
The team is continuing to refine and improve their triage test by adding more diagnostic biomarkers (including directly measuring TB antigens) and multiplexing the assay so that it can detect up to 10 analytes simultaneously.
Additional authors of the paper include Liangxia Xie from the Wyss Institute, BWH, and Tufts University; Margaret Pyle from the University of Maryland Medical Center; Marta Suarez from Daktari Diagnostics; Tobias Broger from the Foundation for Innovative New Diagnostics; Dan Steinberg from Salford Systems; Shaali Ame and Said Ali from Public Health Laboratory-Ivo de Carneri; Marilla Lucero, Diozele Sanvictores, and Veronica Tallo from the Research Institute for Tropical Medicine; Matthew Szucs, Melanie MacMullan, and Steven Carr from the Broad Institute; Frode Berven from the University of Bergen; Arup Dutta, Usha Dhingra, Saikat Deb, and Sunil Sazawal from the Center for Public Health Kinetics in New Delhi; Robert Bencher and Dominic Eisinger from Myriad RBM; Saurabh Mehta from the Cornell Institute for Nutritional Sciences, Global Health, and Technology; Wafaie Fawzi from the Harvard T. H. Chan School of Public Health; Ian Riley from the University of Queensland; Zul Premji from Muhimbili University of Health and Allied Sciences; Robert Black from the Johns Hopkins Bloomberg School of Public Health; Christopher Murray from the University of Washington; and Bill Rodriguez from Draper Richards Kaplan Foundation.
This research was supported by the University of Melbourne and a Grand Challenge in Global Health grant from the Bill & Melinda Gates Foundation.