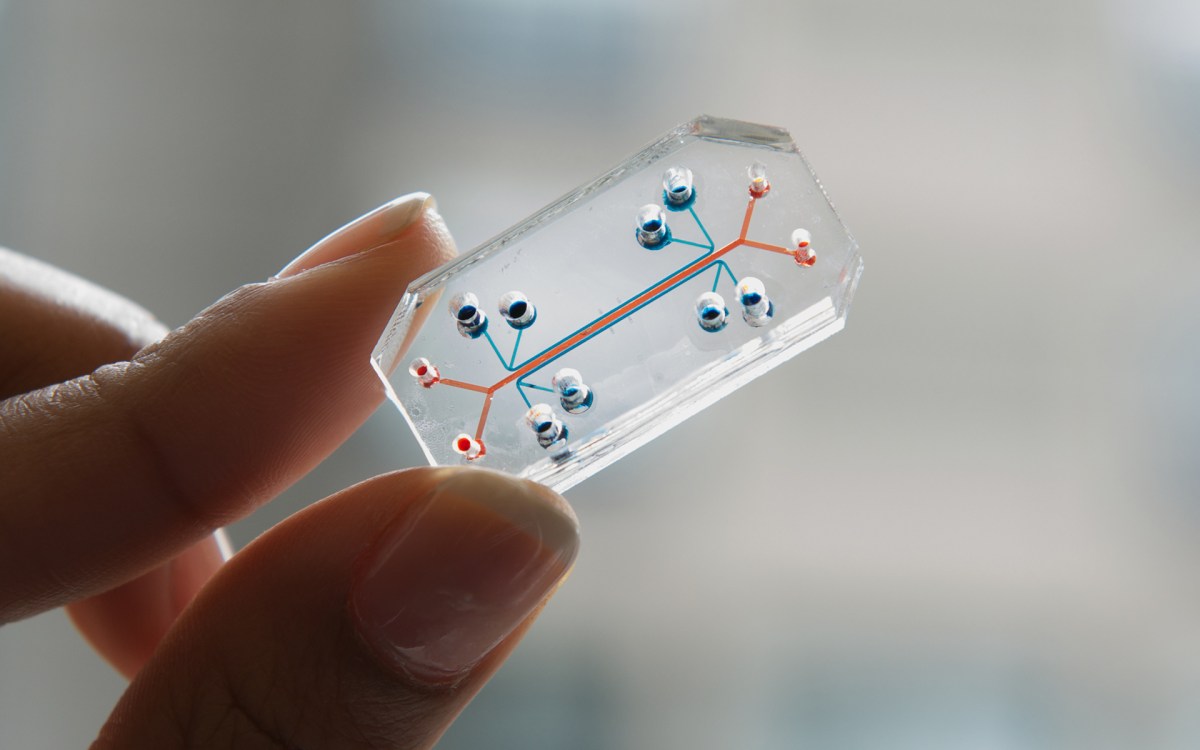

Image: Ocskaymark/Getty Images
Health
A silent epidemic
Geriatrician Sharon Inouye on the need to combat delirium in COVID-19 patients
This is part of our Coronavirus Update series in which Harvard specialists in epidemiology, infectious disease, economics, politics, and other disciplines offer insights into what the latest developments in the COVID-19 outbreak may bring.
Only a few decades ago, medical professionals believed they couldn’t do anything to stop a subset of elderly patients in the hospital from sliding into delirium — an acute state of confusion that can arise from illness or surgery and that raises risk of serious health complications and death.
Then Sharon Inouye proved that delirium is preventable. She created the world’s most widely used checklist to identify delirium and developed a program that hundreds of hospitals have used to reduce cases of the condition by an estimated 40 percent. Inouye is a professor of medicine at Harvard Medical School (HMS) and director of the Aging Brain Center in the Marcus Institute for Aging Research at Hebrew SeniorLife.
Now, after years of progress, Inouye worries that hard-won best practices for reducing delirium risk are getting lost in the turmoil of COVID-19 care.
Early data from peer-reviewed studies suggest that one-third of hospitalized COVID-19 patients of all ages, and two-thirds of those with severe disease, show signs of delirium, said Inouye. For a variety of reasons, some potentially avoidable, delirium management is falling behind, she said. Indeed, the pandemic has led to conditions almost perfectly designed to cause delirium, she said.
That’s concerning to Inouye and colleagues because, as the American Delirium Society explains, patients who experience delirium in the hospital remain hospitalized longer than their peers, have more complications and are more likely to die during their hospital stay or in the following year, need long-term care or develop cognitive impairment, including dementia.
Inouye spoke with Harvard Medicine News about why cases of delirium have risen during the coronavirus pandemic and what clinicians and caregivers can do about it.
Q&A
Sharon Inouye
HMS: What worries you most about elderly populations’ increased susceptibility to the new coronavirus?
Inouye: I have so many worries. If I had to narrow it to my two major concerns, one is what social isolation is doing to all older people, even those who don’t have COVID-19. Older adults who are sheltering at home are not getting exercise, they’re not socializing, a lot are falling into depression, they’re getting weak and frail, and as a consequence there are more falls, more fractures, all kinds of things, such that they need to be hospitalized for non-COVID-19 reasons.
The other issue is that we’re seeing an epidemic of delirium in COVID-19 patients globally, and it’s getting very mismanaged. A lot of that may be unavoidable — when you’re trying to keep someone alive, you may not follow the best practices for delirium prevention, so we can understand that — but I do think from talking to colleagues that some of it is avoidable.
HMS: What may be avoidable and what may not?
Inouye: Reports from around the world indicate a pattern of overuse of chemical restraints such as antipsychotics and other sedating drugs. I think health care providers are feeling very anxious and pressured, so when a patient starts to get agitated, providers get scared for the patient’s safety and their own safety and feel they have to sedate the patient. But sedating them is not always needed and leads to many complications.
I always try to put myself in other people’s shoes. Let’s say your patient has cognitive impairment so it’s hard to explain things to them, they have hearing impairment, they’re fearful, and you’re coming in there all gowned up like a person from outer space and your voice is muffled behind two masks and a face shield and you have to stay six feet away. They can’t see or hear you, they can’t read your lips. They’re confused and frightened. They can’t have a family member there to translate for them or calm them down. It’s like a setup to be a nightmare for an older adult. So your reaction is to reach for the drugs so you can quickly get the IV in, get a COVID-19 swab or a chest X-ray.
I understand why it’s happening, and yet I really believe that if you could just take the extra minute to come close, hold their hand, look in their eyes … Some doctors are taping pictures of themselves to their gowns so patients can see them. Talk to patients and say, “Listen, I know how scary this is. We need to make sure you don’t have this infection, or if you do, that you get the right treatment. So here’s what I’m going to do right now.”
It doesn’t take much extra time. But it’s still time, and doctors and nurses are just not able to do that right now because the volume is so high and the patients are so sick and health care workers are frightened. It’s a perfect storm of not-good things.
And then, if patients do have to be sedated, a lot of the short-acting medications we would normally use have run out, so doctors are having to use drips of benzodiazepines, which under normal circumstances you would never give to older patients, or they’re using general anesthesia because there aren’t any other options. It’s not how anyone would want to practice.
“We need to be aware of the damage of social isolation in older adults as well. As human beings, we need connection. It’s so important for our survival.”

HMS: Can anything even be done to prevent delirium if someone’s on a ventilator?
Inouye: There’s a lot you can do. Getting people up and walking reduces the risk of delirium, and there are protocols for walking people even when they’e on a ventilator. Some ICUs are doing that because studies show that walking raises oxygen saturation and gets patients off ventilators faster, which frees up the machines for other patients. It takes three staff members to help with the walking, but it can be done.
In the ICU, you can lower delirium risk by preserving the sleep/wake cycle, such as by making the room dark and quiet at night and providing earplugs and eye masks. You can play soothing music. You can cycle medications (when medications are available). For those who are sedated, you can lighten the sedation periodically. You can have orientation boards up in the room to help patients remember where they are. You can help them communicate through writing or pointing. Some ICUs have developed therapeutic activities like fun games to keep the mind active. It’s not ideal when someone can’t be in the room regularly because of isolation precautions, but there still is a lot that can be done.
And for COVID-19 patients who are not in the ICU, the regular delirium prevention checklist still applies. Other considerations include facilitating remote visits with family members, minimizing drugs associated with confusion, avoiding physical restraints, providing vision and hearing aids as needed and attending to nutrition and hydration.
HMS: What resources are available?
Inouye: Our Hospital Elder Life Program, or HELP, has created a website about COVID-19 and delirium. It includes a patient toolkit, delirium screening and management guidance, tools for advance care planning during the pandemic, help with social isolation and more. Within a week, people had translated the toolkit materials into Spanish and Portuguese.
It’s also been wonderful to see new ways hospitals have devised to connect patients with family members and the outside world in secure ways. People are so creative in times of crisis. Everybody is reaching out and helping one another.
HMS: What information is emerging about how many COVID-19 patients experience delirium?
Inouye: The two best pieces of evidence I’ve found are a JAMA Neurology paper from April 10 on the neurologic manifestations of COVID-19 in China and an NEJM paper from April 15 on neurologic features in severe COVID-19. The JAMA study reported mental status change in 30 percent of patients, and the NEJM study found an even higher rate, with mental status change in 65 percent of patients and agitation in 69 percent. Both of those probably represent delirium. And that’s in all ages, not only older adults.
HMS: Is it too early to tell to what extent delirium may arise from the coronavirus itself versus the hospital environment?
Inouye: It’s not clear yet, but it’s likely a combination.
There’s some evidence of direct invasion of the brain by the coronavirus. The loss of smell is probably from a direct invasion of the olfactory nerve, and that connects directly to the frontal lobes. The NEJM article showed some light-up of the meningeal space, which could be another sign of viral encroachment into the brain. In addition, there appears to be some vascular involvement, where the coronavirus increases people’s risk of stroke. That could be another etiology for delirium. And as you may have seen in the news, the virus can instigate a cytokine storm — a severe amount of inflammation — and a lot of those patients do very poorly.
On top of those, you have all the sedatives and other drugs that can contribute to delirium.
Then, as a result of delirium, people become immobilized and deconditioned, which in turn causes a cascade of consequences like pressure ulcers, falls, urinary tract infections, increased risk of dementia … That’s my fear: that it’s not just delirium, it’s all these really bad long-term outcomes.
HMS: Can the worst outcomes be avoided?
Inouye: I’m hoping we can change it. We need to get on a better path with the management of delirium. We need to minimize the use of these sedating medications when possible. We need to advocate for caregivers to be allowed back at the bedside. Some facilities are letting family members into rooms where patients have both COVID-19 and dementia to reduce risk of delirium, but there are still no-visitor policies in a lot of places. We need to be aware of the damage of social isolation in older adults as well. As human beings, we need connection. It’s so important for our survival.
HMS: What else gives you hope?
Inouye: If there is a silver lining to this pandemic, it’s that people are seeing how important delirium is. There may never have been this much delirium all at one time. I think it’ll raise awareness. And when we can let our breath out and have time to educate everyone again, at least we will have strategies and resources and training in place for the future.
This interview was edited for length and clarity.
To hear more about delirium and Inouye’s life and career, listen to our podcast, recorded several months before the SARS-CoV-2 pandemic emerged.