Photo illustration by Judy Blomquist/Harvard Staff
Health
A key to the next pandemic: An early-warning system
Solutions
What do we need to do to get ready for the next global pandemic?
A Q&A with Michael Mina
In this series, the Gazette asks Harvard experts for concrete solutions to complex problems. Michael Mina is assistant professor of epidemiology at the Harvard T.H. Chan School of Public Health, a member of the School’s Center for Communicable Disease Dynamics, and associate medical director in clinical microbiology at Brigham and Women’s Hospital’s Pathology Department. Mina’s work revolves around disease testing and the development of new technologies to better understand the population and immunological consequences and patterns underlying infectious diseases.
GAZETTE: Is it possible to prevent the next pandemic? If not, can we better prepare for it?
MINA: Pandemics are going to happen, but we can absolutely prevent the devastation that occurs from a pandemic. We can act now to put us in a position so that when the next pandemic does happen, we don’t have to allow it to get out of control. We can build tools to find it quickly and to act fast. We can build up new public health infrastructure to tackle it once it starts spreading.
There are a lot of ways to do this. One of those steps is building up proper surveillance. We can work together — across countries — in a way that betters societies everywhere. We didn’t see it in this pandemic, unfortunately, primarily because our president couldn’t even unite people in one country. But in what I would consider more ordinary times, a virus should be something that all people on earth can rally around.
GAZETTE: What would such a surveillance system look like?
MINA: An immunological observatory, a global immune observatory, would be a massive engineering feat, the likes of which may be compared — at least in my vision — to the weather system. We don’t need physicians working on this problem; we really need engineers and epidemiologists and mathematicians. It would be a “collective global good” sort of program to help prevent — or at least rapidly identify — the next pandemic so that we can respond quickly.
It would run all the time in the background and would allow two things. One would be rapid identification of new infectious diseases. It would be a massive, everyday surveillance program using ready-to-access blood samples from blood banks or hospitals that are about to be thrown away — there are tons of ways to get blood samples in the world. This could be supported by federal governments or by industry or the Department of Defense. It would be a daily churn, running lots of different tests to look at people’s immune responses.
GAZETTE: From those immune responses, we’d know what is circulating out there?
MINA: I think of every individual as a recording device. We’re all just USB sticks, always recording. The problem is that it’s really hard to uncover what we have recorded. But we have the tools to actually go into our blood and say, “What has Michael recorded today in terms of infectious disease exposures? He didn’t get sick, but maybe he got exposed to something.” We could start doing that for millions of people every single day. That would create a robust surveillance program. The constantly recording devices of our immune system would be interpreted and read out, “Hey, it looks like there’s a new coronavirus spreading in Wuhan.” Or, in late January [2020], “It looks like there are some people with what looks like a new virus popping up in New York City.” And then you would read the news and say, “There’s a coronavirus outbreak in Wuhan,” put two and two together, and Governor [Andrew] Cuomo would have had the firepower to close down the city in early February instead of March. That would have saved tens of thousands of lives and perhaps prevented that major outbreak in New York.
“We can act now to put us in a position so that when the next pandemic does happen, we don’t have to allow it to get out of control,” says Michael Mina.
Jon Chase/Harvard Staff Photographer

GAZETTE: The key would be that we’re not waiting for people to get sick or for someone to notice that several people have gotten sick with something that they don’t recognize? It would be a routine scan of people’s blood collected for other procedures?
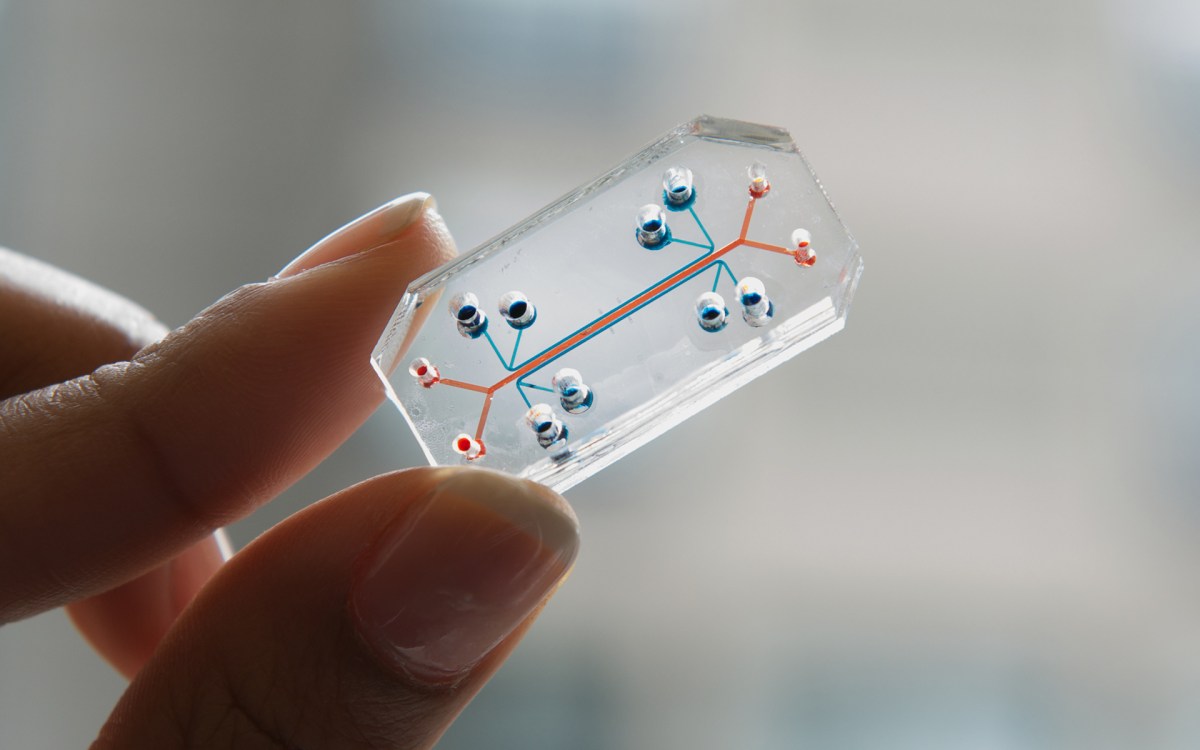
MINA: Yes. We have tools that we are developing in my lab, some initially invented by collaborators like Steve Elledge [Gregor Mendel Professor of Genetics and of Medicine] here at Harvard, that use a drop of blood, just a finger prick. The government could spend a few hundred million dollars and buy every American 10 of these that they could use throughout the year — it’s like filter paper and a lancet. These things could be mailed to everyone’s homes. We actually did this in Massachusetts recently. We mailed thousands of people a little piece of filter paper and a little finger prick thing, just like a diabetes finger prick device, and you put a drop on the filter paper, mail it back into the lab. And with that one drop, we can evaluate somebody’s blood for hundreds of thousands of distinct antibodies simultaneously.
What we’re doing is asking, for this person: Have they seen any number of hundreds of different pathogens? And we get high resolution for what those individual antibodies look like. For example, if you get a COVID antibody test, you get one number back. With our technology, you get 1,000 numbers back just for COVID. So you can start building up something like fingerprints of what different pathogens look like in terms of the immunological response. Then, if there is a novel virus, something the world has never seen before, you can detect it.
We didn’t have this coronavirus in our test a year and a half ago, obviously, because we didn’t know it existed. But we would have very quickly picked it up by seeing a picture from a lot of people that looked like a coronavirus antibody response. Our pattern recognition software would have said, “Hey, we just got these 30 new coronavirus cases and these new antibodies detected in people with coronavirus, but they don’t target the known coronavirus spike protein. Maybe that’s because it’s a new spike protein, and it’s a new coronavirus.” We could use the pattern recognition and the resolution that comes from these new tests to be able to see what are essentially weird patterns. They look a lot like a coronavirus, but don’t quite fit the patterns we’re used to seeing for coronaviruses. That would give us a hint that maybe a new one is spreading.
GAZETTE: What is the status of these tests today?
MINA: These technologies exist and are very cheap. We’ve been trying to build them into a much more robust platform. They could essentially be built into a program that governments or nonprofits could buy and utilize.
It’s an extraordinarily powerful way to try to identify new transmission. We’re doing a pilot right now in partnership with a company called Octapharma. This company collects blood plasma from regular people, so every week my laboratory gets tens of thousands of samples from places all across the United States. There are 110 different sites.
This is a centralized way to get a huge number of specimens. We are processing them for COVID antibodies. In this case, we’re doing passive collection of all these blood samples that were going to be thrown away by the company. So the company said, “We’ll just ship them to you.”
So through 2020, we will have processed around half a million specimens, and we’ll be able to reconstruct the entrance of this virus into the United States and watch, on a practically daily basis, how the virus’ prevalence shifted, grew, and fell, and grew again across the U.S.
Now we’re looking back in time, but what I want to do is to get caught up so that we’re doing it in real time. Then we’ll be able to tell a governor, who might have turned down the state’s testing program for viruses, that our surveillance system is starting to see new cases of flu early this year, or coronavirus, or we are detecting a lot of new antibodies against Lyme disease and it looks like this is going to be a really bad year, or Zika, whatever the virus or pathogen might be.
It can also be used not just for pandemic detection, but to provide a whole new data stream that allows people to say, “There’s really good evidence that there’s rhinovirus moving around in your community.” So, if you’re a parent and your kid is sick, you probably want to know: Does your kid have the flu? Does your kid have adenovirus? Coronavirus? Rhinovirus? RSV? Each of those require different levels of attention.
So maybe you open up your phone, and an app says your community, your ZIP code, has had a lot of rhinovirus over the past week and almost no flu. So you could probably say, “Look, kid, you’re going to be just fine. You very likely have rhinovirus, and if you don’t get much worse, we don’t really have to take action.”
I think of it like the weather system. Right now we look at our phones, and if it says it’s going to rain, we bring an umbrella. We don’t wait until it starts raining. We preemptively take it with us to work.
GAZETTE: And so these two functions would be side by side — surveillance for new pathogens and a more routine state of viral — or whatever — transmission occurring in your area?
MINA: That’s right. It would be serving dual purposes. Maybe the whole program could be funded by subscribers or something like that. I don’t know. I just think that there are ways to make it work. Frankly, it should just be funded by the government. This pandemic is a $16 trillion hit on our economy. If the government put $2 billion into an effort like this and it had any chance at all to stop a major expansion of a new pandemic virus in the future, that’s well worth the investment. The potential benefits greatly outweigh the financial risk.
GAZETTE: We talked about a global surveillance system, but you also mentioned building up public health infrastructure as a way to stay ahead of a future pandemic. What does that look like?
MINA: To not have another 2020, we need to put a few things in place. First really is a playbook. Science isn’t immutable, but science is much more standard than policymakers. We should not be banking on this or that administration — some might be more scientifically savvy than others. There’s no reason we can’t be anticipating this and come up with a playbook that every policymaker, whether it’s governors, presidents, or prime ministers, should be able to open and say, “OK, this is a virus that seems to be spreading quite readily with aerosolized transmission. It has an R naught of around two; it doesn’t seem to be spread too much by fomite transmission; and it’s a coronavirus. Now what is the way to deal with this?”
We should have those playbooks written so that when it happens, we can push a button and say, “OK, these are the things we need in place. These are the potential good approaches to take. And these are the tools we’re going to need.”
GAZETTE: Is this a process that could run, at least initially, independent of political leaders? Insulated from politics?
MINA: I think so. One lesson that we should learn from this pandemic and from the Trump presidency is that though we assume that scientists with the best interests of humanity would be leading efforts, that did not happen in this presidency. We should have an independent crisis group that doesn’t include political appointees. They can say, “This is serious.” It could be a constant group of advisers — not the CDC because the CDC has its daily ongoing work — people who maybe rotate every two years, like a National Guard of scientists. It could be a small group, maybe only 20 or 30 who respond when called upon for a threat.
GAZETTE: What does a strong public health system look like? And how is that different from what we have right now?
MINA: I will answer that question from an infectious disease perspective, because the broader issue of public health is huge and includes nutrition, smoking, and many other things. But it means optimizing the system to help the most people, even at the expense of individuals. Public health tools, whether vaccines, a test, or distancing and masks, need to be evaluated in the context of population and not individual risk.
That requires a whole new way of thinking, and I’d like to start a new field called public health engineering because, ultimately, the response to an outbreak has to be engineered. That’s a big difference. Medicine is very much a one-on-one interaction between a patient and a doctor. It’s not a cold engineering problem. Public health is. It does include consideration of social structures and belief systems, but those are part of the optimization problem.
More like this




GAZETTE: Is this idea of public health at times conflicting with individual well-being something we’ve had the luxury of forgetting, since we’ve tamed so many infectious diseases?
MINA: Absolutely. We have not had to deal with adversity on our shores in any real population-wide way in decades or even longer. We’ve lost track of what it means to act collectively. World War II was a great example of when we said, “We have to work collectively. We have to optimize our response.” By the end of World War II, we were rolling out B24 bombers every 60 minutes. That is something that would have been unfathomable if we were trying to optimize every individual’s safety and well-being and not thinking about the population-level response.
If you go further back and a plague was on board a ship, you’d burn the ship and quarantine every passenger on it. You’d do whatever was needed because the last thing we wanted is for this thing to spread to the population. We’ve advanced from that, but our problem today is that the virus is the same. It doesn’t care. The virus doesn’t feel for our emotions. It’s not an enemy that we can talk down. We can’t bribe a virus with money. It is completely emotionless. There’s nothing we can do to control it, except to control it. I think we have lost all sense of that.
We’re really good in this country at doing biology, at doing medicine. We were able to go from zero to a vaccine finishing phase three trials in months. But we completely fail — always in this country and in many countries — to actually do the public health part. We did all the expensive biological stuff; we did all the fancy stuff that gives people credit, all the doctor-y things, all the technology things. But then when it came to scaling and distributing the vaccine, the not-sexy, public health intervention part, nobody thought about it.
It was complete afterthought, but it’s the most important part. So we need a whole new field that is thinking about public health optimization in a whole new way. We need engineers on the ground.
GAZETTE: How do you get at the human behavior part of this? Getting people to do what science and public health tells us will work?
MINA: One thing that governments do badly is we ignore public health. And the way that we communicate public health to the public needs to change. It needs campaigns that are on par with the campaigns of Joe Camel and Marlboro Man, Doritos and Coca-Cola. When it’s for profit, we have huge industries focused on how to get people to do something they didn’t know they wanted to do. There’s a huge amount of psychology that goes into those ad campaigns and those messaging campaigns. Why is that amazing tool left only to adverse things for human populations? To for-profit things that generally don’t make people healthier?
GAZETTE: Is this maybe a communications aspect of your public health engineering?
MINA: Yes, it all needs to be taken into account. A problem for the spread of rapid tests is that people say, “Well, people won’t know how to use them.” Well, they’ll know how to use them if they see it on the back of every magazine, and they see news anchors and people on sitcoms do a COVID test at home. It absolutely needs to be part of this overall approach to how we tackle pandemics in the future. We should not be shying away from marketing. We should be pouring billions of dollars into McCann and into Coca-Cola’s branding agency. We should be paying them well to tell the public about public health, to teach people. There’s no reason why we can’t do this. It would be well worth every dollar, and probably be some of the best return on investment we could ever put forward, given the context of this pandemic right now.
GAZETTE: Is there an opportunity today in that there is a generation of kids and young adults for whom this will be a formative event in their lives? They may be the ones who get this message even if their elders are more blasé.
MINA: I do think that signs are pointing to a new generation of people more engaged with each other, even if it’s being engaged with each other through technology. I hope that many people will be interested in public policy, in infectious disease dynamics, and epidemics. The interest in going into infectious disease and pandemic research has skyrocketed among young people this year. Around me, anyway, there have been armies of young people — and some older people — who have really rallied around, in this case, me and this idea of rapid testing, building grassroots campaigns online. To see that energy has been pretty heartening.